
Prevalence and Factors Associated with Statin Prescription for Primary Cardiovascular Disease Prevention in Bangkhla Hospital
Article Sidebar
Main Article Content
Abstract
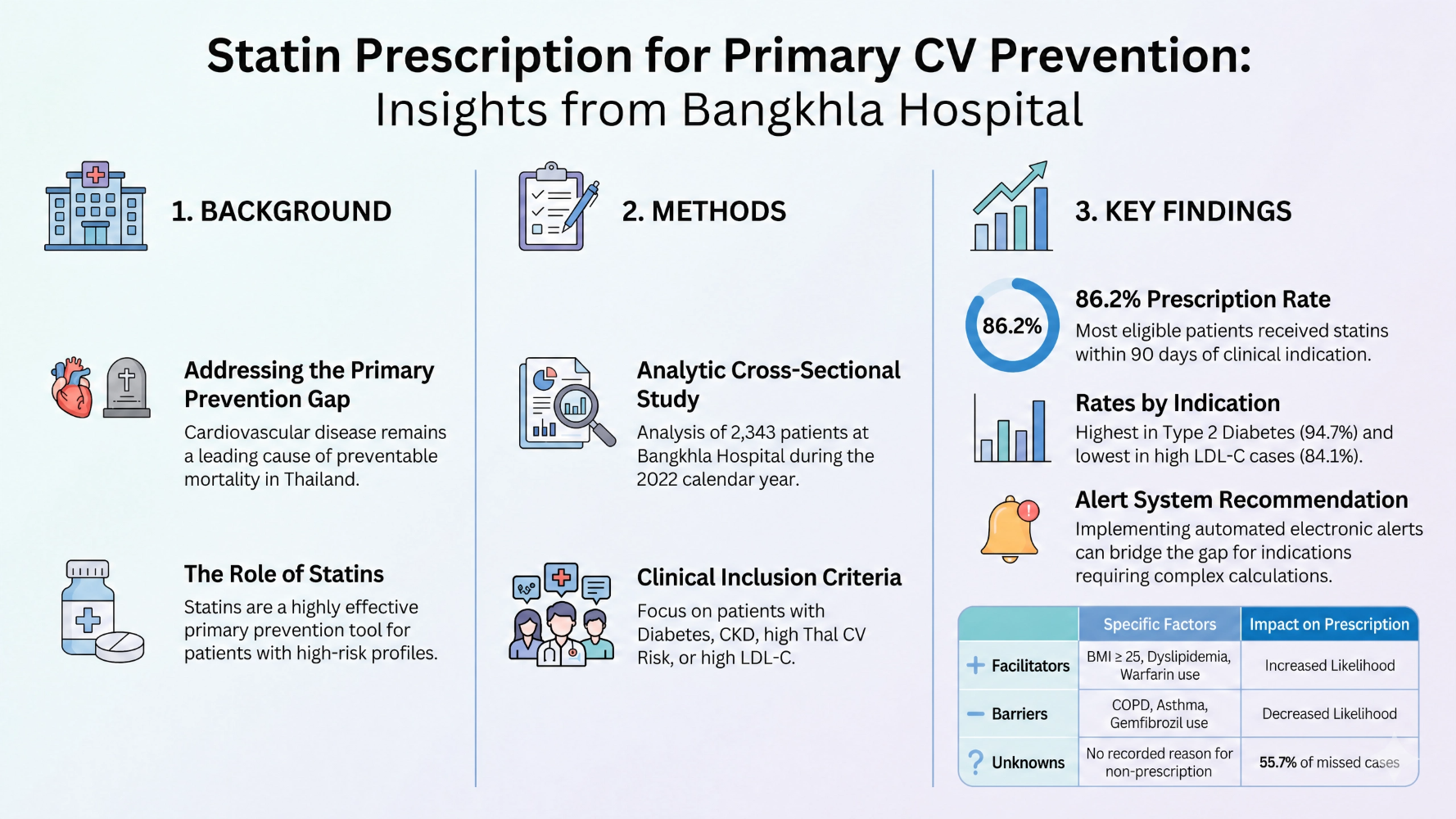
Background: Cardiovascular diseases are preventable, with statins being an effective primary prevention strategy when indicated. However, the national database records lack relevant information, and no prior studies have been conducted at Bangkhla Hospital. Therefore, this study aimed to determine the prescription rate of statins when indicated, identify factors associated with statin prescribing, and examine the reasons for non-prescription.
Design: Analytic cross-sectional study
Methods: This study accessed patient database records at Bangkhla Hospital for individuals with indications for statin therapy as primary prevention in 2022. A minimum sample size of 310 patients was calculated. The primary outcomes of interest included the statin prescription rate among indicated patients, reasons for non-prescription in eligible individuals, and factors associated with statin prescribing. Data were analyzed using percentages, means, and standard deviations. Associations were examined using multiple logistic regression at a significance level of 0.05.
Results: A total of 2,343 patients met the study criteria, and population-based, non-random sampling data were analyzed. Among patients with indications for statin therapy as primary prevention at Bangkhla Hospital, 86.2% received statins within 90 days of indication. Statin prescription rates varied by indication: type 2 diabetes in patients aged ≥ 40 years: 94.7%, chronic kidney disease in patients aged ≥ 50 years: 90.4, patients aged ≥ 35 years with a 10-year Thai CV risk ≥ 10%: 85.6% and patients aged ≥ 21 years with LDL-C ≥ 190 mg/dL: 84.1%. Factors associated with statin prescribing included body mass index ≥ 25.0 kg/m², pre-existing dyslipidemia, warfarin use, higher HDL-C levels, age ≥ 21 years with LDL-C ≥ 190 mg/dL, and type 2 diabetes in patients aged ≥ 40 years.
Conclusions: In 2022, a total of 2,343 patients at Bangkhla Hospital met the criteria for statin therapy as primary prevention for cardiovascular disease, with 86.2% receiving statins. Factors associated with statin prescription included obesity, pre-existing dyslipidemia, warfarin use, higher HDL-C levels, age ≥ 21 years with LDL-C ≥ 190 mg/dL, and type 2 diabetes in patients aged ≥ 40 years. We recommend implementing a prescription alert system for statins in patients who meet the indications.
Keywords: statin, cardiovascular disease, primary prevention, factors
Downloads
Article Details

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
The content and information in articles published in the PCFM journal are solely the opinions and responsibilities of the authors. The journal's editorial board does not necessarily agree with or share any responsibility for them.
All articles, information, content, images, etc., published in the PCFM journal are the copyright of the PCFM journal. If any individual or organization wishes to reproduce, distribute, or use any part or the entirety of the content, they must obtain written permission from the PCFM journal beforehand.
References
กลุ่มยุทธศาสตร์และแผนงาน สำนักโรคไม่ติดต่อ กรมควบคุมโรค. แผนยุทธศาสตร์การป้องกันและควบคุมโรคไม่ติดต่อระดับชาติ 5 ปี (พ.ศ. 2560 - 2564). ใน: กระทรวงสาธารณสุข, บรรณาธิการ. นนทบุรี: อิโมชั่น อาร์ต; 2560.
World Health Organization. The top 10 causes of death: World Health Organization [Internet]. 2020 [cited 2021 Jan. 7]. Available from: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death
สุรพันธ์ สิทธิสุข, อภิชาต สุคนธสรรพ, สุรจิต สุนทรธรรม, ชัยชาญ ดีโรจวงศ์, วรรณี นิธิยานันท์, วันดี โภคะกุล, และคณะ. แนวทางเวชปฏิบัติการใช้ยารักษาภาวะไขมันผิดปกติเพื่อป้องกันโรคหัวใจและหลอดเลือด พ.ศ. 2559. กรุงเทพ-มหานคร: สมาคมโรคหลอดแดงแห่งประเทศไทย; 2560.
Koene RJ, Prizment AE, Blaes A, Konety SH. Shared Risk Factors in Cardiovascular Disease and Cancer. Circulation. 2016;133:1104-14.
Celermajer DS, Chow CK, Marijon E, Anstey NM, Woo KS. Cardiovascular disease in the developing world: prevalences, patterns, and the potential of early disease detection. J Am Coll Cardiol. 2012; 60:1207-16.
Khanam F, Hossain MB, Mistry SK, Afsana K, Rahman M. Prevalence and Risk Factors of Cardiovascular Diseases among Bangladeshi Adults: Findings from a Cross-sectional Study. J Epidemiol Glob Health. 2019;9:176-84.
วิชัย เอกพลากร, หทัยชนก พรรคเจริญ, กนิษฐา ไทยกล้า, วราภรณ์ เสถียรนพเก้า. การสำรวจสุขภาพประชาชนไทยโดยการตรวจร่างกายครั้งที่ 5 พ.ศ. 2557. นนทบุรี: สถาบันวิจัยระบบสาธารณสุข; 2559.
Arnett DK, Blumenthal RS, Albert MA, Buroker AB, Goldberger ZD, Hahn EJ, et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;140(11):e596-e646. PubMed PMID: 30879355
Grundy SM, Stone NJ, Bailey AL, Beam C, Birtcher KK, Blumenthal RS, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2019;73: e285-e350.
Mach F, Baigent C, Catapano AL, Koskinas KC, Casula M, Badimon L, et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020;41:111-88.
Cannon CP, Blazing MA, Giugliano RP, McCagg A, White JA, Theroux P, et al. Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes. N Engl J Med. 2015;372:2387-97.
Collins R, Reith C, Emberson J, Armitage J, Baigent C, Blackwell L, et al. Interpretation of the evidence for the efficacy and safety of statin therapy. The Lancet. 2016;388(10059):2532-61.
Schwartz GG, Steg PG, Szarek M, Bhatt DL, Bittner VA, Diaz R, et al. Alirocumab and Cardiovascular Outcomes after Acute Coronary Syndrome. N Engl J Med. 2018;379:2097-107.
Teramoto T. Extending the “Lower is Better” Principle to Japanese and Possibly Other Asian Populations. Circulation. 2018;137:2010-2.
Adhyaru BB, Jacobson TA. Safety and efficacy of statin therapy. Nat Rev Cardiol. 2018;15:757-69.
Ciffone NA, Copple T. Managing dyslipidemia for CVD prevention: A review of recent clinical practice guidelines. Nurse Pract. 2019;44:8-16.
Cosentino F, Grant PJ, Aboyans V, Bailey CJ, Ceriello A, Delgado V, et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J. 2020;41:255-323.
Ferro CJ, Mark PB, Kanbay M, Sarafidis P, Heine GH, Rossignol P, et al. Lipid management in patients with chronic kidney disease. Nat Rev Nephrol. 2018; 14:727-49.
Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170 000 participants in 26 randomised trials. The Lancet. 2010;376(9753):1670-81.
Armitage J, Baigent C, Barnes E, Betteridge DJ, Blackwell L, Blazing M, et al. Efficacy and safety of statin therapy in older people: a meta-analysis of individual participant data from 28 randomised controlled trials. Lancet. 2019;393(10170):407-15.
Ridker PM, Danielson E, Fonseca FA, Genest J, Gotto AM, Jr., Kastelein JJ, et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med. 2008;359:2195-207.
Homer K, Boomla K, Hull S, Dostal I, Mathur R, Robson J. Statin prescribing for primary prevention of cardiovascular disease: a cross-sectional, observational study. Br J Gen Pract. 2015;65(637):e538-44.
McBride CL, Akeroyd JM, Ramsey DJ, Nambi V, Nasir K, Michos ED, et al. Statin prescription rates and their facility-level variation in patients with peripheral artery disease and ischemic cerebrovascular disease: Insights from the Department of Veterans Affairs. Vasc Med. 2018;23:232-40.
กระทรวงสาธารณสุข. ข้อมูลเพื่อตอบสนอง Service Plan สาขาไต [รายงานมาตรฐาน]. กระทรวงสาธารณสุข [อินเทอร์เน็ต]; 2564 [เข้าถึงเมื่อ 24 ม.ค. 2564]. เข้าถึงได้จาก: https://hdcservice.moph.go.th/hdc/reports/page.php?cat_id=e71a73a77b1474e63b71bccf727009ce
กระทรวงสาธารณสุข. ผู้ป่วยกลุ่มเสี่ยงต่อโรคหลอดเลือดและหัวใจได้รับยากลุ่ม Statin เขตสุขภาพที่ 6 จังหวัดฉะเชิงเทรา ปี งบประมาณ2563: กระทรวงสาธารณสุข [อินเทอร์เน็ต]. 2563 [เข้าถึงเมื่อ 24 ม.ค. 2564]. เข้าถึงได้จาก: https://hdcservice.moph.go.th/hdc/reports/report.php?source=pformated/format1.php&cat_id=e71a73a77b1474e63b71bccf727009ce&id=cc417db46c6b7f713a205b27fec159bd
กระทรวงสาธารณสุข. ผู้ป่วยกลุ่มเสี่ยงต่อโรคหลอดเลือดและหัวใจได้รับยากลุ่ม Statin เขตสุขภาพที่ 6 จังหวัดฉะเชิงเทรา ปี งบประมาณ2564: กระทรวงสาธารณสุข [อินเทอร์เน็ต]. 2564 [เข้าถึงเมื่อ 24 ม.ค. 2564]. เข้าถึงได้จาก: https://hdcservice.moph.go.th/hdc/reports/report.php?source=pformated/format1.php&cat_id=e71a73a77b1474e63b71bccf727009ce&id=cc417db46c6b7f713a205b27fec159bd
Daniel WW. Biostatistics: A Foundation for Analysis in the Health Sciences. New York: Wiley; 2009.
Matthias AT, Nihari Padmasiri MS, Kavindi Somathilake BGG, Wijesekara Pathirana NS. Clinical inertia in lipid screening and prescribing statins for primary prevention. International Journal of Noncommunicable Diseases. 2021;6:187-92.
สุรพันธ์ สิทธิสุข, สุรจิต สุนทรธรรม, วรรณี นิธิยานันท์, รุ่งโรจน์ กฤตยพงษ์, วีรพันธุ์ โขวิฑูรกิจ, ประวีณ โล่ห์เลขา, และคณะ. แนวทางเวชปฏิบัติการบำบัดภาวะไขมันผิดปกติในเลือดเพื่อป้องกันโรคหัวใจและหลอดเลือด พ.ศ. 2567. ใน: ประวีณ โล่ห์เลขา, สุรจิต สุนทรธรรม, บรรณาธิการ. กรุงเทพมหานคร: ราชวิทยาลัยอายุรแพทย์แห่งประเทศไทย ในพระบรมราชูปถัมภ์; 2567.
แนวทางการป้องกันและรักษาภาวะแทรกซ้อนของหลอดเลือดหัวใจ และหลอดเลือดสมอง. แนวทางเวชปฏิบัติสำหรับโรคเบาหวาน 2566. พิมพ์ครั้งที่ 2. กรุงเทพมหานคร: สมาคมโรคเบาหวานแห่งประเทศไทย; 2567.
Van Gelder IC, Rienstra M, Bunting KV, Casado-Arroyo R, Caso V, Crijns HJGM, et al. 2024 ESC Guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): Developed by the task force for the management of atrial fibrillation of the European Society of Cardiology (ESC), with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Endorsed by the European Stroke Organisation (ESO). European Heart Journal. 2024;45:3314-414.
